My diagnosis is something called an intractable migraine, or you could also call it an Energizer bunny migraine. In my case, it’s been going and going and going for four months without responding to treatments. Though that sounds bad (and it is), my experience 24/7 is that of a simple headache, not a migraine, because I’m on so many medications that are supposed to keep the rest of the migraine symptoms contained. But various things cause the migraine to flare up anyway, like certain foods. Or lack of sleep. Or sunny days. Or skipping acupuncture. Or stepping on a crack in the sidewalk. Or breathing air.
Many people have asked what my “average” day with an intractable migraine is like, but because I’m always on the edge of a flare up, any single day of an intractable migraine is impossible to describe. It’s not like I have just a headache from nine until noon, then take a break for lunch, then get a migraine flare until five, then pack up my things and go home for a quiet evening. Every day is spent with me at the mercy of the migraine’s whims, and January in particular has been a month of much migraine whimsy. In fact, half of this month so far has been spent with migraine flares, and some are worse than others. So, this post will instead give you glimpses of what the past month has been like for me, in an attempt to give you some insight into my crazy, light-sensitive life.
My average migraine flare this month starts with either dizziness or a sudden throbbing headache or ice pick headache attack. Within an hour or two, I am also lethargic and nauseous, and sitting in bed with a cup of tea, my phone to play music, and a coloring book. I can be stuck in bed for days, completely uninterested in moving or eating, in the dark. I’ll leave the house only to go to medical appointments…which means I have to leave the house nearly every day. Chronic pain is a schedule obliterator. I have three weekly appointments: acupuncture, physical therapy, and plain old therapy. On top of that, I work with a neurologist, a pain neurologist, a GI doctor, a primary care physician, an integrative medicine doctor, and an orthodontist (because even though my braces are off, they can always come up with something else I simply must do). That’s six specialists, and each is scheduled every 4-6 weeks, meaning I see at least one of them every week in addition to my three regularly scheduled weekly appointments. If I’m not having a migraine flare, I drive myself to my appointments, which are scattered all across the city. Fortunately, I love driving and solving parking puzzles. But if I am having a flare, and I’m lucky, Cory or a friend drives me. If I’m having a flare and am not lucky, I have to take a Lyft. The Lyft rides are hard because you never know how smooth the ride is going to be, so I keep my eyes closed under my sunglasses and hope for the best. I don’t open my eyes when wearing sunglasses, because if the sun is behind me and reflects off the back of the glasses into my eye, it sends pain shooting through my head.
If I can’t get a migraine flare to stop, or if any of the aforementioned things occurs during a flare (I eat the wrong food, or I don’t sleep, or I step on a sidewalk crack, etc.), it turns into a monster. The most recent one was last week on Friday night. Cory went straight to the grocery store after work, then came home and made us dinner. As soon as I finished eating dinner, I was doubled over and unable to move without feeling miserable. My headache kept flaring to the point that I was crying out in pain every few minutes. There was nothing to do but get myself to bed, pop some pills, secure an ice pack, and wait. For the first three months, medications didn’t help at all. But now they sometimes help, and sometimes don’t.
There is one thing that always helps, though: acupuncture. Acupuncture is the most anticipated appointment on my calendar every week, because when it comes to cool packs and needles, my acupuncturist spares no expense. The average appointment involves six needles in the back of my head, two in the front, and ten more in my neck and shoulders. He pushes them in until the muscles twitch to release tension, which in turn flares my headache and usually makes me yell. But it’s no pain, no gain in the acupuncture world, and there is a lot of gain to be had in my case. First off, the acupuncture treatments are the only thing that can get me instantly out of a migraine flare. If I’m having a flare during my usual appointment, or if he fits me in last minute for an extra, my amazing acupuncturist throws needles, cool packs, and heated blankets at the problem for hours. I’ve come out feeling so great every time this happens, and so hungry. In fact, I often go straight from acupuncture to a coffee shop to buy a large slice of banana bread and a peppermint tea (because I couldn’t eat bananas for a long time, and peppermint tea is my new vice after giving up afternoon coffee). The second benefit of getting lots of needles in my head is the opportunity to chat with my acupuncturist. He shows more creativity than any doctor when it comes to managing pain; he’s suggested everything from snorting peppermint oil to doing things I love in order to rob my nervous system of pain sensations. He also takes pity on my clueless-ness, me being so young and ignorant of how the medical system works. We discuss what my various specialists are telling me to do, and he helps me reason through the information and prioritize my next treatments.
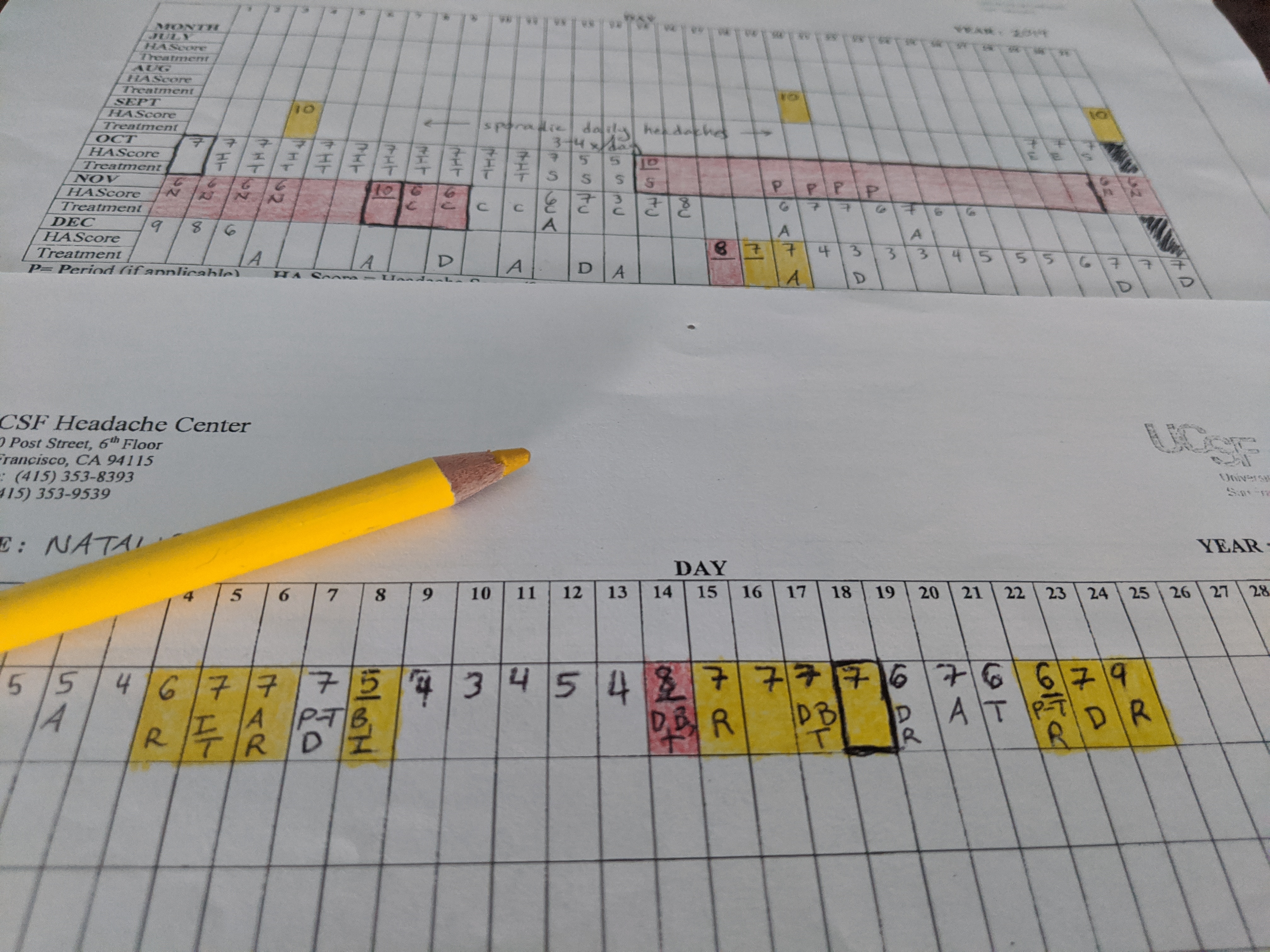
This is what my month looked like, medically. I had flares that are short, flares that are long. I went to specialists, I spent lots of time with my acupuncturist. But there were also a few days this month with no migraine flare and no appointments. And those days were probably more similar to yours- they are what one might call normal days. These were the days when I felt well enough to go outside and actually enjoy the sunshine instead of hiding from it, sometimes well enough to get out on my bike. I used these days, or these pieces of days, to visit friends and get physical activity, to empty the dishwasher and do laundry, to write and play the piano. I also ate a lot, because food tastes so amazing when I’m not nauseous.
I loved these days. But even these good days didn’t feel normal, not the normal sort of normal. I still had a headache on these days, and I still was shoving my migraine down using lots of pills. So the good days really felt like occasional, exhausted Saturdays after weeks full of Wednesdays, and before more weeks that might be all Wednesdays, too. Not enough time to get away from life, not enough time to really recover. But they were enough to get a taste, a reminder of what I’m aiming for- I’m aiming for these “good” days to soon be the worst days I have.
So I’m finishing January with a whimper, not a shout, and perhaps with a migraine flare. But here’s to hoping for better, and believing this is just a phase. And having real hope, hope that doesn’t fade when my migraine flares, is what gives me peace as I color the day away, go to my fourth doctor for the week, and do my best to enjoy each Saturday in a month full of Wednesdays.

